

Drug Demand Reduction
Introduction
The Anti Narcotics Force is a unique organization as it not only deals with interdiction of narcotics but also carries out demand reduction activities. Most of the countries in the world have separate organizations for enforcement measures and for demand reduction. In accordance with the UN Conventions on the subject, the Government of Pakistan has set up a Ministry to deal with the multi dimensional activities associated with the use of illegal drugs.
The Drug Abuse Prevention Resource Centre is one of the two directorates of the Anti Narcotics Force dealing with demand reduction measures since 1998. Previously DDR was a project (from 1988 to 1998) funded by different international donors from time to time i.e European Commission,(1988- 1989), US Aid (1991-1992) and joint E.C./GOP Project (1995-1998) for carrying out the activities of drug demand reduction. Finally it became a part of ANF in 1998.
Functions
- Preparation and implementation of projects / programmes in relation to drug prevention / demand reduction.
- Maintaining liaison with national and international organizations connected with research into drug abuse issues for collecting and disseminating research findings and other information abuse / demand reduction issues.
- Develop pool of expertise within the DDR in order to provide meaningful assistance for demand reduction activities to Regional Directorates of ANF, Provincial Government Agencies, NGOs/CBOs and others.
- Creating a body of resource persons all over the country who can help in national effort in drug abuse prevention / demand reduction.
- Arranging for audiovisual and printed materials to support training and other drug abuse prevention activities.
- Development and implementation of a media policy regarding drug abuse prevention / demand reduction.
- Maintaining lists of NGOs /CBOs, assisting these and networking them.
- MARTC.
- Co-ordination with the UNDP/WHO/UNDCP/US-NAS and DAP of Colombo Plan and all other International Organizations/Foreign Missions.
- Co-ordination of SAARC Drug Prevention Activities/Seminar/Workshops as Focal Point.
- To liaise with Provincial Governments on Matters of Registration of Drug Addicts as required under Section 52 of the Control of Narcotics Substance Act-1977.
- Matters relating to Treatment and Rehabilitation, Establishment of Treatment/ Detoxification facilities at the Federal Level as required under Section 53 of the CNS Act 1977.
DRUG INFORMATION
Opium
Papaver somniferum var. album, is the species of plant from which opium and poppy seeds are extracted. Opium is the source of many opiates, including morphine, thebaine, codeine, papaverine, and noscapine. The plant itself is also valuable for ornamental purposes, and has been known as the "common garden poppy", referencing all the group of poppy plants.
Derivatives of Opium
i) Morphine:
Morphine is an extremely potent opiate analgesic psychoactive drug, is the principal active ingredient in Papaver somniferum (opium poppy, or simply opium), is considered to be the prototypical opioid. In clinical medicine, morphine is regarded as the gold standard, or benchmark, of analgesics used to relieve severe or agonizing pain and suffering.
ii) Heroin:
Heroin and Opium are derived from poppy plant. Heroin, or diacetylmorphine, also known as diamorphine, is a synthesized from morphine, a derivative of the opium poppy. Heroin is used as both a pain-killer and a recreational drug. Frequent and regular administration is associated with tolerance, moderate physical dependence, and severe psychological dependence.
Manufacturing
Heroin, also known as diacetyl morphine is produced from acetylation of morphine derived from natural opium sources. Numerous mechanical and chemical means are used to purify the final product.
Methods of Use
Heroin, also known as diacetyl morphine is produced from acetylation of morphine derived from natural opium sources. Numerous mechanical and chemical means are used to purify the final product.
- One of the most common methods of illicit heroin use is via intravenous injection.
- May administer the drug through snorting.
- Smoking by inhaling its vapors when heated; either with tobacco in a rolled cigarette or by heating the drug on aluminum foil from underneath.
Effects
Intravenous users typically experience the rush within 7 to 8 seconds after injection, while intramuscular injection produces a slower onset of this euphoric feeling, taking 5 to 8 minutes. When heroin is sniffed or smoked, the peak effects of the drug are usually felt within 10 to 15 minutes. In addition to the initial feeling of euphoria, the short-term effects of heroin include a warm flushing of the skin, dry mouth, and heavy extremities. Chronic users may develop collapsed veins, infection of the heart lining and valves, abscesses, cellulites, and liver disease. Pulmonary complications, including various types of pneumonia, may result from the poor health condition of the abuser, as well as from heroin's depressing effects on respiration.
Cannabis
Derivatives of Cannabis
i) Hashish
It is derived from female cannabis (Hemp/Bhang) plant. Hashish is a preparation of cannabis composed of the compressed stalked resin glands called trichomes, collected from the cannabis plant (Bhang). Hashish is often a solid or paste-like substance of varying hardness and pliability, and will soften under heat. Its color can vary from green, yellow, black, reddish brown, or most commonly light to dark brown.
Manufacturing
Hashish is made from cannabinoid-rich glandular hairs known as trichomes, as well as varying amounts of cannabis flower and leaf fragments. The flowers of a mature female plant contain the most trichomes, though trichomes are found on other parts of the plant. The resin reservoirs of the trichomes, sometimes erroneously called pollen are separated from the plant through various methods. The resulting powder is compressed into blocks of hashish aided by heat, which can be easily stored and transported.
ii) Marijuana
Marijuana is the most commonly abused illicit drug. A dry, shredded green/brown mix of flowers, stems, seeds, and leaves of the plant Cannabis sativa, it usually is smoked as a cigarette (joint, nail), or in a pipe (bong). It also is smoked in blunts, which are cigars that have been emptied of tobacco and refilled with marijuana, often in combination with another drug. It might also be mixed in food or brewed as a tea. As a more concentrated, resinous form it is called hashish and, as a sticky black liquid, hash oil. Marijuana smoke has a pungent and distinctive, usually sweet-and-sour odor.
ii) Effects
When marijuana is smoked, its effects begin immediately after the drug enters the brain. Smoking marijuana deposits several times more THC into the blood than does eating or drinking the drug. Within a few minutes after inhaling marijuana smoke, an individual�s heart begins beating more rapidly, the bronchial passages relax and become enlarged, and blood vessels in the eyes expand, making the eyes look red. A marijuana user may experience pleasant sensations, colors and sounds may seem more intense, and time appears to pass very slowly. The user�s mouth feels dry, and he or she may suddenly become very hungry and thirsty. His or her hands may tremble and grow cold.
Coca Leaf
Derivatives of Coca Leaf
Cocaine
It is derived from Coca leaf. Cocaine is a powerfully addictive stimulant that directly affects the brain. Cocaine is not a new drug. and coca leaves, the source of cocaine, have been ingested for thousands of years. Pure cocaine was first extracted from the leaf of the Erythroxylon coca bush, which grows primarily in Peru and Bolivia, in the mid-19th century. The powdered, hydrochloride salt form of cocaine can be snorted or dissolved in water and injected. Crack is cocaine that has not been neutralized by an acid to make the hydrochloride salt. This form of cocaine comes in a rock crystal that can be heated and its vapors smoked. The term �crack� refers to the crackling sound heard when it is heated.
Effects
Cocaine is a powerfully addictive drug. Cocaine�s effects appear almost immediately after a single dose, and disappear within a few minutes or hours. Taken in small amounts (up to 100 mg), cocaine usually makes the user feel euphoric, energetic, talkative, and mentally alert, especially to the sensations of sight, sound, and touch. It can also temporarily decrease the need for food and sleep. Some users find that the drug helps them perform simple physical and intellectual tasks more quickly, while others experience the opposite effect.
Psychotropic Substances
Derivatives
Ecstasy (MDMA)
MDMA (3,4-methylenedioxymethamphetamine) is a synthetic, psychoactive drug chemically similar to the stimulant methamphetamine and the hallucinogen mescaline. MDMA is an illegal drug that acts as both a stimulant and psychedelic, producing an energizing effect, as well as distortions in time and perception and enhanced enjoyment from tactile experiences. Adolescents and young adults use it to promote euphoria, feelings of closeness, empathy, sexuality and to reduce inhibitions. It is considered a "party drug" and obtained at "rave" or "techno" parties. Although MDMA is known universally among users as ecstasy, researchers have determined that many ecstasy tablets contain not only MDMA but also a number of other drugs or drug combinations.
Methamphetamine
Today, methamphetamine is second only to alcohol and marijuana as the drug used most frequently in many Western and Midwestern states. Seizures of dangerous laboratory materials have increased dramatically. Methamphetamine is a highly addictive drug with potent central nervous system stimulant properties. In the 1960s, methamphetamine pharmaceutical products were widely available and extensively diverted and abused.
Buprenorphine
Buprenorphine is a semi-synthetic opiate with partial agonist actions at the antagonist actions at other opioid receptors. Buprenorphine hydrochloride was first marketed in the 1980s by Reckitt & Colman (now Reckitt Benckiser) as an analgesic, available generally as Temgesic 0.2 mg sublingual tablets, and as Buprenex in a 0.3 mg/ml injectable formulation. In October 2002, the Food and Drug Administration (FDA) of the United States of America additionally approved Suboxone and Subutex, buprenorphine's high-dose sublingual pill preparations for opioid addiction, and as such the drug is now also used for this purpose.
Use
Buprenorphine is also used recreationally, typically by opioid users. Users sometimes report a feeling of general well being, perhaps even to the point that they may become more outgoing or talkative. Due to the high potency of tablet forms of buprenorphine, only a small amount of the drug need be ingested to achieve the desired effects. The buprenorphine preparation, Suboxone, comes in an orange lemon-lime flavored tablet for sublingual administration. The taste of Suboxone is described by some to be very unpleasant. Subutex is unflavored and very bitter.
Effects
Common adverse drug reactions associated with the use of buprenorphine are similar to those of other opioids and include: nausea and vomiting, drowsiness, dizziness, headache, itch and dry. The most severe and serious adverse reaction associated with opioid use in general is respiratory depression, the mechanism behind fatal overdose. Buprenorphine behaves differently than other opioids in this respect, as it shows a ceiling effect for respiratory depression.
DRUG ABUSE SCENARIO
National drug abuse assessment 2006 / 07
United Nation Office on Drugs and Crime (UNODC) in collaboration with the Ministry of Narcotics Control, Anti Narcotics Force, carried out a National Drug Abuse Assessment 2006/07. The report on this Assessment contains data of opioid users and also highlights statistics and analysis of patterns and trends in drug abuse in Pakistan.
Factors responsible for increase of drug abuse in Pakistan
- Increased availability of drugs at low prices.
- Rapidly changing social norms which place new demands on individuals for which drugs offer a false solution.
- Lack of jobs and economic frustration.
- Lack of proper interest in education, peer pressure and negligence of parents.
- Existence and operation of drug dens.
- Lack of drug education within the family and in educational institutions.
- Apathy on the part of community leaders in responding to drug abuse symptoms.
Drug of choice
- Hashish (cannabis) is the most commonly used substance
- Sedatives and Tranquilizers
- Heroin
- Opium
- Injecting drug use
- Ecstasy
- Solvent Abuse among Street Children
What are Opioids
- Opium
- Heroin
- Buprenorphine, Sosegon, Codeine, Morphine, Pentazocine are Synthetic Opioids
Opioid users (estimated number of 628,000 opioid users in Pakistan)
- Heroin Users: Heroin remained the most popular drug being abused by 77% or approximately 484,000. These findings mirror those of Drug Abuse Assessment undertaken in 2000 (estimated number of heroin users in 2000 drug abuse assessment was 500,000). Given the massive increase of opium and heroin production in neighboring Afghanistan this stability in prevalent rates is a notable achievement.
- Age Group: The opioid users fall in the age bracket of 15-64 years which is very high rate.
Drug injecting users
- Over the last one decade the drug abuse problem has become more complicated as the number of IDUs has doubled. There are an estimated 125,000 injecting drug users
- It is important to note that in the year 2000 the absolute number of injecting drug users in Pakistan was 60,000, which almost doubled in 2006, an alarming trend that needs to be addressed on priority
- In 1990�s the proportion of injecting users was reported between 2 and 8 percent of opiod users
- In 2000 injecting was reported among 15 percent (60,000)
- In 2006 up to 29 percent (125,000) injected drugs
Major drugs of use
- Cannabis is the most commonly used substance followed by sedatives and tranquilizers, such as benzodiazepines, heroin, opium and other opiates
- Ecstasy & cocaine (ATS) are emerging drugs especially among youth belonging to the higher socio-economic groups in some urban centres in Pakistan
- Inhalant abuse is common among street children
Initiation of drug
- Average age of initiation of drug use is 18 years
- Majority of drug users interviewed had used Charas (Cannabis) as the first substance in their lifetime
Reasons of starting drugs
- Influence of friends or peer pressure
- Social and family stresses
- Sibling or other family member�s use of drugs
- To heighten sexual pleasure
- To overcome frustrations/tragedies
- As pain medication
ANF HOSPITALS - MODEL ADDICTS TREATMENT & REHABILITATION CENTRES (MATRCs)
The treatment and rehabilitation of drug addicts can be defined as a journey from drug dependence to a healthy, drug - free lifestyle. The process is long and painful. Addicts need maximum assistance and care to be able to abstain from drugs and to break the addictive cycle, hence the need for comprehensive treatment and rehabilitation programmes that conform to the biological, psychological and social needs of individuals. Hence the requirement of a separate specialized and independent centres/hospital for the drug abusing population.
ANF is maintainng following hospitals:
In Pakistan, majority of existing treatment and rehabilitation facilities provide detoxification services only, particularly in the public sector run health facilities, and no rehabilitation programmes exist. All district hospitals are mandated to have one ward exclusively for treatment of drug addicts. These wards however only provide detoxification facilities. Rehabilitation programmes are extremely costly and demand highly motivated people to take care of drug addicts and their particular circumstances. To cater for needs of hundreds of thousands of heroin addicts alone, is beyond the capacity of any organization. Since rehabilitation, particularly in Pakistan, would imply job assessment, job training, job placement, employment etc, the difficulties involved under the given social circumstances are imaginable.
As per section 52 and 53 of CNSA Act 1997 the responsibility for the registration and rehabilitation of drug addicts falls within the purview of the Provincial Government. However to provide quality treatment and meet the growing deficiency of treatment facilities the Anti Narcotics force, has undertaken the following measures:-/
- Setting up of Model Addiction Treatment and Rehabilitation Centres: Islamabad, Quetta & Karachi.
- Two Model Addiction Treatment & Rehabilitation Centres were established at Islamabad and Quetta.
- The projects started in July 2004.
- Both were 20 bedded centres providing free treatment, food, boarding and rehabilitation to drug addicts.
- Efforts were also made for their job placement.
- In July 2007 the centres were upgraded to 45 beds.
- Third Model Addiction Treatment & Rehabilitation Centre � Benazir Shaheed ANF Hospital� has been established on May 2010 at Karachi. It is a 60 bedded hospital.
Vision, Mission & Objectives
Vision
Drugs free Society through Advocacy, Primary Prevention and Best Practices in Treatment and Rehabilitation.
Mission
Ensure best possible service directly and indirectly to reduce the drugs Demand and providing professional support in maintaining the recovery process to prevent the recurring relapse, ensuring reduction of supply.
Objectives
- Detoxification and rehabilitation facility to drug addicts.
- Minimizing the risk of relapse and re-integration of the recovering addicts in the society.
- Rehabilitation and vocational training to the detoxified addicts.
- Enabling the addicts to be self reliance.
- Be the valuable parts of the societal machinery.
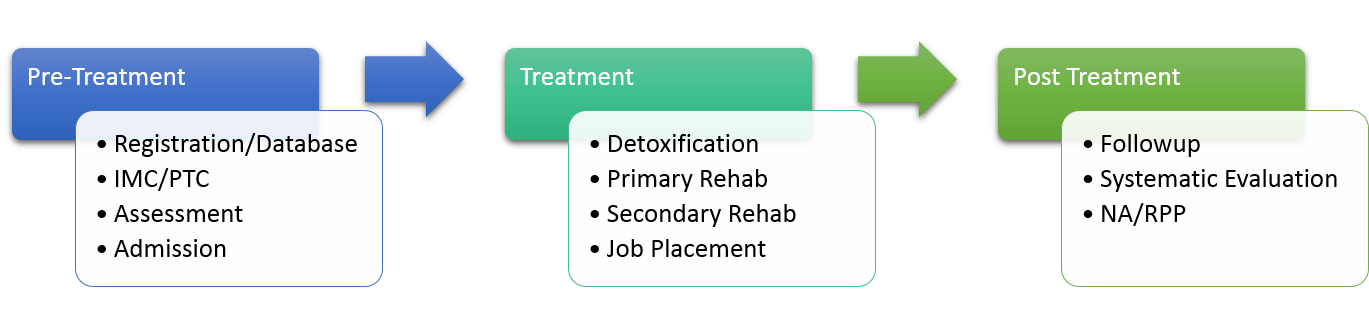
Treatment Methodology
Registration Procedure
Following steps will be followed:-
- Personal appearance at near MATRC with a family member.
- Availability of CNIC and Photo.
- Filling of initial detail.
- Issuing of registration token.
Following baseline tests will be completed:-
- Blood CP with ESR.
- Serum urea creatinine.
- X-ray chest with Report.
- Urine R/E.
- HBs. Ag and Anti HCV.
- Phone call on the number provided at the time of registration.
- Personal appearance with a family member.
- Checking of the required Lab tests.
- Photo session.
- Initial assessment.
- Informed consent signed by, patient, family, duty staff member and finally the Project Manager.
Note: In case of known TB, Cardiac issue, HBs, Ag, Physical Disability, severe surgical issue and patients with psychotic (Schizophrenia, major depression, suicidal tendencies and mentally retarded) are not recommended for admission. They are referred to other hospitals (PIMS or BBH, Rawalpindi)
Following are the requirements for admission:-